IntroductionTranscranial magnetic stimulation (TMS) induces electric fields (E-fields) that propagate through white matter pathways, influencing distributed brain networks beyond the stimulation site. Deep TMS using the H7 coil is an FDA-cleared treatment for obsessive-compulsive disorder (OCD), targeting the medial prefrontal cortex (mPFC) and anterior cingulate cortex (ACC), key nodes of the cortico-striato-thalamo-cortical (CSTC) circuit. However, how individual differences in E-field distribution and network propagation contribute to clinical response remains unclear. We hypothesized that a dose-dependent local neuronal response, amplified through structural connectivity, predicts treatment outcome following deep TMS in OCD.
MethodsTwenty-two patients with OCD received 6 weeks of TMS (20 Hz, 100% rMT) targeting the mPFC/ACC. Individual E-field distributions were computed and averaged within 90 AAL brain regions. Network activation was modeled as A = (I − αC)
-1 r, where C is the structural connectome, α is the network coupling strength, and r = f(e; β, θ) represents the local neuronal response to E-field magnitude e. Four neuronal response models were evaluated: excitatory/inhibitory sigmoid, exponential decay, and biphasic. (α, β, θ) were optimized across CSTC ROIs via leave-one-subject-out cross-validation. Predicted network activation was correlated with percentage improvement on the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS, Spearman).
ResultsAcross four candidate neuronal response models, only the biphasic model yielded a cross-validated prediction that survived FDR correction (Fig. 1). Network activation within the left superior orbital frontal region was positively correlated with percentage Y-BOCS improvement (r = 0.65, p_fdr = 0.012). The optimized parameters (β = 0.189, θ = 37.78, α = 0.879) defined an optimal E-field window of ~20–38 V/m; stimulation beyond this range produces reduced neuronal responses. The strong coupling (α = 0.879) indicates local effects are greatly amplified through structural connectivity. Parameter estimates were highly stable across LOSO folds (interquartile range = 0 for all parameters).
DiscussionThese findings suggest that individual differences in therapeutic response to deep TMS may depend on both local E-field magnitude and its propagation through long-range structural networks. Furthermore, the left frontal superior orbital region might be an effective TMS target for OCD treatment. The biphasic dose-response suggests an optimal E-field window for therapeutic stimulation. Below this window, stimulation is insufficient to drive meaningful neuronal responses; above it, excessive E-field likely reduces neuronal output, forming an inverted-U dose-response relationship. Together, these results support a network-based framework for the mechanisms of deep TMS in OCD and highlight the importance of individualized E-field optimization.
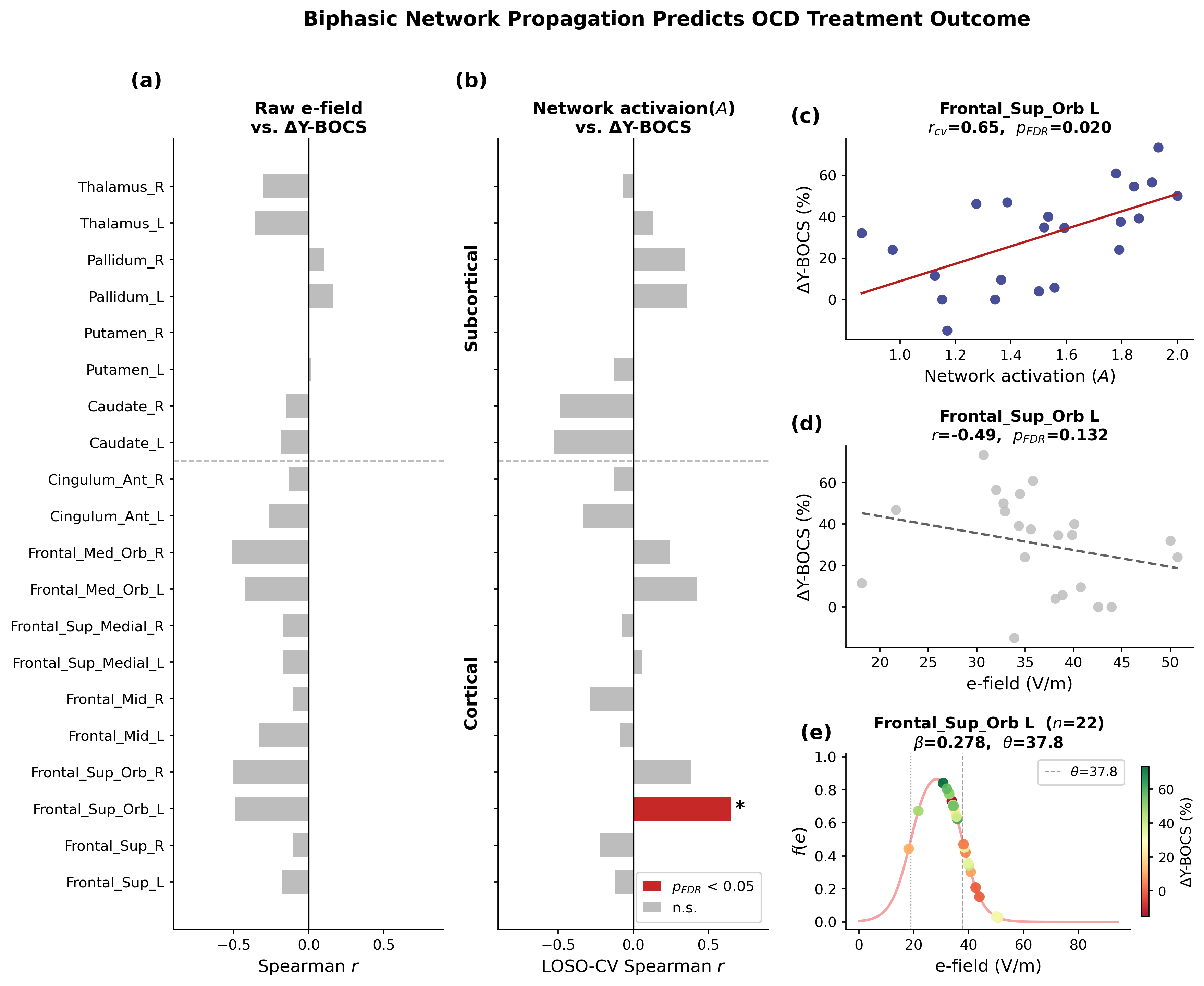 Figure 1. Correlations between E-field/network activation and clinical outcome in the CSTC ROIs. (a) Raw E-field showed no significant correlations. (b) The biphasic neuronal response model identified the left superior orbital frontal cortex as significantly associated with percentage Y-BOCS improvement. (c-f) Network activation/raw E-field correlation maps, and fitted biphasic neuronal response f
Figure 1. Correlations between E-field/network activation and clinical outcome in the CSTC ROIs. (a) Raw E-field showed no significant correlations. (b) The biphasic neuronal response model identified the left superior orbital frontal cortex as significantly associated with percentage Y-BOCS improvement. (c-f) Network activation/raw E-field correlation maps, and fitted biphasic neuronal response f
References1. Harel, M., Perini, I., Kämpe, R., Alyagon, U., Shalev, H., Besser, I., ... & Zangen, A. (2022). Repetitive transcranial magnetic stimulation in alcohol dependence: a randomized, double-blind, sham-controlled proof-of-concept trial targeting the medial prefrontal and anterior cingulate cortices. Biological psychiatry, 91(12), 1061-1069.
2. Burguiere, E., Monteiro, P., Mallet, L., Feng, G., & Graybiel, A. M. (2015). Striatal circuits, habits, and implications for obsessive–compulsive disorder. Current opinion in neurobiology, 30, 59-65.
AcknowledgementNo
